
Memory, Stigma, Future Challenges
Published on 01/12/2025

In 2024, 1.3 million people contracted HIV, 40.8 million were living with the virus, and 630,000 died from AIDS-related illnesses. These figures are in addition to the 92.3 million people in total who’ve been infected since the start of the pandemic, according to estimates.
More than forty years have passed since the first cases were detected and, although steady progress has been made, we still can’t class HIV as a disease of the past.
So what have we learned after four decades of fighting HIV? What stigma does it carry today? Which scientific challenges remain to be solved? And what social transformations are essential to envisage an AIDS-free future?
On the occasion of World AIDS Day, and coinciding with the release of the documentary RED: Una cronología del VIH de la mano de sus protagonistas (RED: A chronology of HIV through the eyes of its protagonists), produced in collaboration with IrsiCaixa and available on CaixaForum+, we spoke to researcher Beatriz Mothe Pujadas and artist Samuel Perea-Díaz to approach HIV from different but complementary perspectives: the scientific search for a cure and the need to look at the disease with new eyes.
MEMORY
What is HIV?
The term HIV defines both the infection and the virus that causes it: the Human Immunodeficiency Virus.
It’s an infection, transmitted via the blood and semen, vaginal and rectal secretions, that attacks and destroys CD4 cells, a type of white blood cell essential for fighting infection and the development of various types of cancer.
Without treatment, HIV progresses in three stages:
- Acute stage (2-4 weeks), in which flu-like symptoms appear and the virus replicates rapidly in the blood, making the risk of transmission very high.
- Chronic stage (asymptomatic), in which it continues to replicate but more slowly.
- Final stage, AIDS (Acquired Immunodeficiency Syndrome), over the course of 10 or more years. People at this stage have severely weakened immune systems that make them prone to AIDS-defining conditions, such as weight and muscle loss, severe infection and cancer. Once in this stage, life expectancy is around 3 years.
Today, thanks to antiretroviral treatment, it’s been possible to prevent the progression of AIDS, reducing the virus to undetectable levels in the blood, where it remains hidden in so-called latent HIV reservoirs.
Where did HIV come from?
The first recorded case of AIDS was in the United States in 1981. It was Gaëtan Dugas, a homosexual flight attendant who became known (mistakenly) as “patient zero“.
In early studies and publications on AIDS, Dugas was accused of being promiscuous and irresponsible, as well as “playing a key role in spreading the virus across the United States”. Thus, HIV became known as “the gay plague.” Years later, the term would evolve to GRID (Gay-Related Immune Deficiency), the 4H disease (Homosexuals, Heroin Addicts, Haemophiliacs and Haitians) and, finally, AIDS (Acquired Immunodeficiency Syndrome).
Studies published years later indicated that Dugas was far from being the source of the pandemic: the virus had been circulating in America for 10 years, and the first verified case dated back to 1959 in the Democratic Republic of Congo.
In fact, genetic evidence indicates that HIV already existed in chimpanzee species in Central Africa, and that transmission to humans began through hunting and handling their meat. Trade routes, as well as the expansion of large African cities and the lack of medical infrastructures, allowed for the rapid (and initially silent) spread of the virus. In the 1960s, Haitian doctors who travelled to the Congo for vaccination campaigns unwittingly contributed to the spread of infection by using shared syringes. Upon returning to Haiti, where there was a major plasma donation centre and which, at the time, was considered a “sexual paradise”, the virus found an ideal setting to reach the United States and eventually become the global pandemic we know today.
A scientific revolution
At first, there was a complete lack of knowledge about the disease. “Early HIV research was driven by urgency” explains Beatriz Mothe Pujadas, an immunology researcher at IrsiCaixa. “The absolute priority was to curb the extremely high mortality rate from an unknown virus“. Efforts focused on developing antiviral drugs and on understanding how the immune system responded in order to slow down the progression of the infection. It was a race against time”.

Beatriz Mothe Pujadas, researcher at the IrsiCaixa centre, Badalona
Today, the scientific landscape has advanced, achieving milestones that once seemed unthinkable:
- “The first milestone, without doubt, was the arrival of ART (antiretroviral therapy) in the mid-1990s” explains Beatriz. “It transformed a fatal disease into a manageable one, making the virus ‘undetectable in the blood‘”.
This was a turning point for patients. “We know that, if the virus is undetectable, it’s also untransmittable (Undetectable = Untransmittable, U=U). This allows people with HIV to live their sexual lives as normal and ensures they can have children without the risk of transmitting the virus to the baby, whilst we also stop the infection from progressing to AIDS”.
- “Another crucial milestone has been the emergence of the first people to be considered ‘cured'” explains Beatriz. This was achieved through transplants of HIV-resistant stem cells, i.e. cells that lack the receptor necessary for the virus to spread. However, this procedure can’t be rolled out to the general population due to the risks associated with transplants.
“Although these are exceptional cases, they demonstrated that a cure wasn’t some kind of scientific utopia but a real possibility. They opened up new lines of research and gave a huge boost to the field”.
- “In the area of prevention, one milestone was the discovery that very simple combinations of antiretroviral drugs can be used to prevent HIV infection. This is known as PrEP (pre-exposure prophylaxis). Although it’s currently the most effective preventive tool, in the future we hope to achieve even more powerful strategies, such as an effective preventive vaccine“.
- “More recently, new long-acting antiretroviral treatments are changing the treatment paradigm: we’ve gone from several pills a day to just one, and now to injectables that last for months. This considerably enhances the quality of life of people with HIV, who have to undergo a life-long chronic treatment”.
“From a broader perspective, there’s one very important turning point: the speed at which we’ve advanced” adds Beatriz. “In 40 years, we’ve gone from not understanding what was happening to having very powerful treatments and preventive strategies. Now it’s no longer just a question of prolonging life but of improving its quality and moving towards strategies that eliminate or silence the virus in a lasting way. That progress, in such a short time, is extraordinary“.
STIGMA
A cultural perspective
There’s still a great deal of stigma towards people with HIV, with damaging results. According to UNAIDS, 25% of people with HIV experienced discrimination when seeking medical care in the past year, and the figures are even higher in already stigmatised groups such as sex workers, transgender people, homosexuals and drug users.
In fact, in 2019 there were still 48 countries with restrictive laws regarding HIV: including mandatory testing in order to obtain entry, residence, work or study permits and, in some cases, even deportation based on serological status. These measures, widely criticised as human rights violations, are based on the false idea that mobility spreads the virus.
A scientific perspective
“At first, the disease created uncertainty and that spread to the whole of society, including the medical community” Beatriz continues. “Very few professionals dared to work with these patients or to investigate the disease. Those who did were true pioneers, such as Bonaventura Clotet. In many centres, people with HIV were relegated to specific wards or spaces because the rest of the hospital avoided sharing spaces for fear of contagion. It was a very difficult situation”.
In 1995, at the peak of the epidemic in Spain, ”la Caixa” Foundation made a bold and decisive commitment to support the fight against AIDS. Together with the Catalan government, it promoted the creation of IrsiCaixa, which is still led today by Dr. Bonaventura Clotet. This was a pioneering initiative at a particularly difficult time for patients, when HIV was taboo, perceived as an inevitably fatal diagnosis and carried a double stigma associated with drug use, certain sexual practices or diseases such as hepatitis and tuberculosis.
“But it was precisely in this hostile context that something extraordinary emerged: an absolutely unique doctor-patient relationship“ explains Beatriz. “The relationship became deeply human, almost one of shared resistance. Clinicians saw the suffering, loss and stigma up close, and this led to a personal involvement that forever changed our approach to HIV care and research. I believe this connection was one of the forces that were driving the science and helping to sustain an entire community that felt abandoned” she adds.
“Today, the perception of HIV within the scientific community has changed a great deal. The taboos have gone but there’s less attention, perhaps because we no longer perceive it as an emergency. But we can’t give up: the pandemic is still ongoing, especially in low-income countries. Furthermore,” concludes Beatriz “the social stigma towards people with HIV is still very much present and that’s a challenge which science alone can’t solve“.
An artistic perspective
“HIV isn’t just a biomedical crisis; it’s an ‘epidemic of meanings'” says artist and “la Caixa” Foundation fellow Samuel Perea-Díaz. “Its artistic representation, key to raising awareness of the reality of the pandemic and to challenging stigma, has always been controversial”.
“In the 1980s and 1990s in the West, the art related to HIV was marked by grief, anger and political urgency. The focus was on the sick body, death, loss and the denunciation of institutional negligence. The slogan Silence = Death encapsulated the need to turn pain into public action” recalls Samuel.
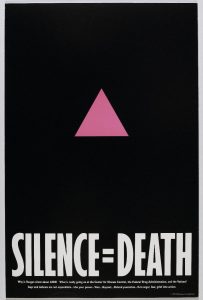
SILENCE = DEATH poster, 1987. Produced by The Silence =Death Project collective. Image from the Brooklyn Museum
Today, access to treatment and the U=U principle have transformed the cultural and artistic narrative. “Now art, without abandoning its political dimension, explores more intimate territories: desire, sexuality, emotional alliances and ways of living with the virus on a daily basis“. For Samuel, “this opens up new aesthetic and political possibilities for thinking about HIV based on the present”.
This perspective underpins Viral Intimacies, the exhibition co-curated by the artist at the nGbK in Berlin alongside a transdisciplinary team. The project is based on a shared premise: “to go beyond the strictly biomedical narrative of HIV and see it as a relational phenomenon—political, social, and intimate” explains Samuel.
One of the central aspects of the exhibition was to decolonise the history of AIDS. “The debate has been narrated almost exclusively from the Global North” Samuel points out. “The exhibition seeks to displace these hegemonic interpretations in order to incorporate global perspectives and, at the same time, to recognise the colonial roots of the epidemic“. As pointed out by co-curator Ahmed Awadalla, the socio-political conditions that enabled the transmission of the virus to humans were heavily influenced by the colonial practices in Africa.
This approach resulted in an exhibition that foregrounded marginalised voices and experiences: “from the prison activism of black women in the US to the stigma linked to access to treatment in Latin America, and the surveillance and pathologisation of racialised queer bodies in Europe” notes Samuel.
Samuel’s own work delves deeper into this genealogy. His doctoral research maps artistic sound responses to the pandemic, influenced by the political activism and intergenerational listening of the late 1980s: “collectives such as ACT UP and Gran Fury, which transformed outrage into public and performative action; and the vocal radicalism of Diamanda Galás, capable of activating memories and mourning through her sound and performances”.
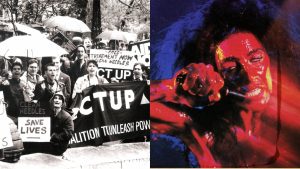
Left: ACT UP demonstration in Hall Park, 1988. Courtesy of Lee Snider. Right: Diamanda Galás on the cover of the album “Masque of the Red Death”, 1988. Credits: Far Out.
That same pulse runs through Hearing Silence, Samuel’s sound installation within the exhibition. “Using data from UNAIDS, the work transforms the data on deaths into sound pulses emitted at 20 kHz, a frequency at the threshold of human hearing: audible, but barely perceptible” explains Samuel. “The aim is for visitors to experience the difficulty of hearing something that’s not immediately present. The pulses act as a spectral trace of lives that aren’t always counted or remembered. By making us aware of these absences, we witness something invisible but real“.

Samuel Perea-Díaz at the installation Hearing Silence, exhibited at Viral Intimacies, nGbK, Berlin. Photograph by Jörg Dedering.
FUTURE CHALLENGES
Thinking about the future of HIV/AIDS involves, as Samuel points out, “moving between hope and political reality”. After four decades of scientific advances and social transformations, the future can’t be constructed without critically reviewing the history of the epidemic, a history that has too often left out those living in the most vulnerable situations. Salvaging their voices, and ensuring they’re not silenced again, is a prerequisite to designing any possible future.
Added to this narrative and cultural dimension are urgent challenges in the political and social spheres. “The political challenge is to move towards the total decriminalisation of HIV and to guarantee sustained funding for social and health programmes. And the social challenge is to eradicate stigma and discrimination“.
In the scientific field, there are two major frontiers: the development of an effective preventive vaccine and the elimination of the latent HIV reservoir, that “hiding place” where HIV remains inaccessible to treatment. “Until we know how to eliminate it or keep it under control in the long term, we can’t claim to have found a functional cure” explains Beatriz. “Although it’s not yet a reality, the advances made in recent years are bringing us ever closer to a tangible solution, which is paradoxical given the reduction in funding for research”.
The 95-95-95 targets proposed by UNAIDS, to help end the AIDS epidemic by 2030, sum up the overall challenge: to diagnose, treat and achieve undetectable viral loads in 95% of the people with HIV. But achieving that goal will depend, as Samuel points out, “on our ability to sustain both activism and investment, ensuring that advances don’t just continue to be made but that they reach all communities”.
“From a scientific point of view, I’m optimistic” notes Beatriz. “We’ll continue to improve treatments and preventive strategies and, hopefully, progress towards a functional cure. But when I think about the future I really want, I imagine a future without stigma. If we could achieve that, if people living with HIV could do so without fear, without prejudice and without added social burdens, that would already represent a huge change. That’s the future I’d like to see“.